
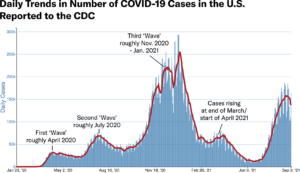
We are now more than a year and a half into the global pandemic of SARS-CoV-2. It’s hard to imagine that what started out as “just a couple of weeks” to crush the curve as we were hoping in March 2020 has resulted in multiple waves of disease and nearly 650,000 deaths in the U.S. (In 18 months, we have suffered more deaths in our country than both World Wars and the Korean and Vietnam wars combined — a fact that makes one stop to catch a breath.)
This novel coronavirus has intermittently paralyzed the globe in fits and starts and, at this point, it continues to barrel through certain regions at a varying pace. What is remarkable and reassuring is that the scientific world has come to the table to advance technology around effective therapeutics and vaccines that render this disease less powerful. We are certain now that vaccination, while not entirely protective against infection, CAN prevent severe illness, hospitalizations, and death – a tremendous feat amidst the otherwise unsettling news of ongoing disease transmission both in our country and around the globe. With higher vaccination uptake, there will be less disease transmission and then a greater chance for all of us to recover to a point where the infection is more nuisance than threat. With combined natural immunity from infection plus vaccine immunity, it’s likely that the swells of infection will become less and less – and our lives can return to some level of pre-pandemic normalcy.
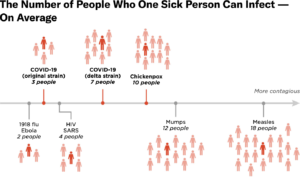
In the U.S., we are currently gripped by the Delta variant (lineage B.1.617.2) which is wreaking havoc particularly in our Southern states. This variant has proven to be hyper-transmissible, and those left unvaccinated across the country have been the most affected by its transmission dynamics. In the immediate future, we hope to use all known mitigation measures plus vaccination to protect those vulnerable and to curb transmission yet again. Below, we answer some frequently asked questions about how we got here and where we go now.
While the Delta variant currently makes up 99 percent of U.S. cases, what are the concerns for future variants, and how can we collectively work to tamp down the risk of variants?
Each day we are hearing of new variants. C.1.2 was identified in South Africa in May 2021. It has been found thus far in Africa, Europe, and Asia. This variant also has potential for hyper-transmissibility and reduced response to vaccines. It is being studied closely regarding whether it may have any advantage over the current Delta variant. Thus far, it’s not even considered a variant of interest — but there is attention here to see if it has any outcompeting potential over the Delta variant.
First noted in Colombia in January, the Mu variant (B.1.621) has been classified as a variant of interest. Mu does have mutations that suggest risk of resistance to vaccines — currently this is present in 39 percent in Colombia, and the WHO is keeping an eye on its trajectory. About 2,000 Mu cases have been identified in the U.S., with most cases noted in California, Florida, Texas, and New York.
“A main goal for us as a nation and worldwide will be to increase vaccination rates to help reduce disease transmission, thus making it harder for the virus to find new hosts.”
Ultimately, a main goal for us as a nation and worldwide will be to increase vaccination rates to help reduce disease transmission, thus making it harder for the virus to find new hosts. To put it in another way, as long as people remain unvaccinated, there will be risk for ongoing viral transmission and risk for potential further mutations. Our hope is that while we continue to increase vaccination rates in the U.S. (which is still only 53 percent fully vaccinated), we also pivot to sharing vaccines, as able, across the globe to reach countries that have less access to vaccines.
Bottom line: While variants should not come as a surprise to us with the spread of a novel viral illness, we do have tools to help prevent further variant production.
Is the Delta variant more virulent?
While the full scope of the imprint left by the Delta variant is still being researched, we do have some data that there is a higher rate of hospitalization with the Delta variant than with the previously dominant Alpha variant (B.1.1.7). According to a report in The Lancet Infectious Diseases, the estimated risk of hospital admission was two times higher for individuals diagnosed with the Delta variant. An important note here: this did pertain to those mostly unvaccinated or partially vaccinated.
On September 3, the CDC released data that from June 20 – August 14, 2021, while Delta was widely circulating, hospitalizations among unvaccinated adolescents was also ten times higher than those fully vaccinated — another testament to the power of vaccines.
What happened in the U.S. to create our current step backwards?
In my opinion, the backwards place we’ve gone in the pandemic since August stems from the perfect storm of three events:
1) The arrival of the hyper-transmissible Delta variant in early spring.
2) Poor timing to relax the masking mandate and other non-pharmaceutical interventions around the same time in mid-to-late May.
3) Perhaps the added concern of vaccine immunity beginning to shift, with those elderly and high-risk groups having been vaccinated in January and February.
What is the current status of breakthrough infections during the surge with the Delta variant?
The messaging via the CDC is now very clear: breakthrough infections are expected. In fact, as of August 19 in L.A. County, breakthrough infections were noted to be 30 percent of all new COVID cases. So while we now understand that COVID-19 vaccine efficacy against infection seems to have declined with the Delta variant, the vaccines are still highly effective against infection leading to hospitalization.
While we are improving our vaccination numbers across the country (47 percent of the U.S. population is still unvaccinated, including our children), I continue to encourage mask-wearing, especially in crowded indoor spaces. We now understand that fully vaccinated people can still get infection and pass that infection along to the unvaccinated and vulnerable – this is the transmission we would hope to prevent in the near term by using masks as another layer of transmission prevention.
When should we be getting in line for additional doses or boosters?
On August 23, 2021, the U.S. FDA gave full approval to COMIRNATY (Pfizer mRNA COVID-19 vaccine) for use in those 16 years and older. It is still under Emergency Use Authorization for those 12-15 years old.
It is also now recommended to give a third dose (or additional dose) to those 12 years and over with certain immunocompromising conditions. We are strictly advised at this time to stay with the same dose series that one had prior for this additional dose (whether that is Pfizer or Moderna). Mix-and-match trials are underway, but it is not advised at this time.
This week the CDC’s Advisory Committee on Immunization reported that they feel more data is needed before recommending boosters widely. There was an announcement regarding rolling out booster shots starting September 20 to those who are vulnerable (elderly) and health care workers who were generally vaccinated early on in January and February. The final vote on this has not yet been authorized by the FDA or the ACIP. On September 17, 2021, the FDA has a scheduled meeting of its Vaccines and Related Biological Products Advisory committee to discuss the issue further.
To complicate matters further around boosters, it may be that Pfizer authorization for the booster dose may come prior to Moderna’s. In fact, there is ongoing discussion and review regarding the booster for Moderna being only 50 micrograms (half of the original doses in the series.) Stay tuned here, and please review with your physician prior to scheduling your booster shot.
The top priority for boosters will be to prevent severe disease in high-risk people. It has also been discussed that the official COVID vaccination series will indeed be a three shot series — this will be determined in the coming months.
Bottom line: We are waiting for the final say on timing and dosage of boosters for the general population.
How should we approach COVID-19 testing?
Since late July it has been well-established that breakthrough infections are happening and there is a risk of transmitting disease to others. Testing, regardless of vaccination status, has become important once again.
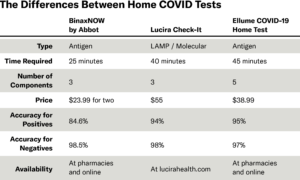
Rapid antigen tests (Ellume and BinaxNow) are now widely available over-the-counter. False positive or false negative testing can be problematic with any rapid test and needs to be backed up with a laboratory-based PCR test, as usual. Rapid molecular tests such as Lucira and Cue Health tests may be slightly more sensitive, but are harder to come by at this time.
Bottom line on testing: regardless of vaccination status, at this time, please test if you are having symptoms, and notify your physician of your status. Isolate if positive and especially to protect those vulnerable around you. Eventually, when enough community immunity is established, I believe these measures will be less important — but for now, isolation with a positive test is required.
(Links: Binax, Lucira, Ellume)
What do the next eight weeks hold? And how do things look going into 2022?
We all feel a great sense of disappointment after our few weeks of moderate normalcy in the early spring prior to Delta’s arrival here in the U.S. One thing that I hope is universally understood at this time is that while one area of our country (or the world, for that matter) is suffering with widespread disease transmission, the rest of us will need to pause and review how we might be able to help control local disease transmission rates by masking and pursuing vaccination. Any area of heightened disease transmission may lead to further variant production, so stopping transmission is paramount.
“The nature and trajectory of a new highly transmissible respiratory illness is not easy to predict, as we well know by now.”
The trajectory of the Delta variant across the U.S. remains to be seen this fall. While the devastating surge in the South may be tapering a bit, the country is necessarily prioritizing our kids’ returning to in-person classes. We are hoping that the return to school does not spur increases in infection rates across the U.S.
With proper layered mitigation measures — including masking, proper ventilation, hand hygiene, and vaccination for those who are able — we may be able to keep cases and hospitalization rates low enough to productively proceed through the remainder of our year, functioning at a level that allows some semblance of normalcy.
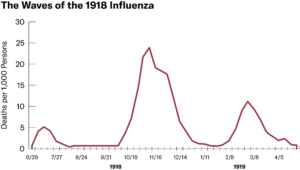
We have to remind ourselves that during the last historic influenza pandemic of 1918, it took about two years to wane, with similar epidemiologic curves as we are experiencing now. The nature and trajectory of a new highly transmissible respiratory illness is not easy to predict, as we well know by now.
Hopefully in the coming year, there will be enough “community” immunity, both natural and vaccine-induced, to render SARS-CoV-2 an endemic disease with only minimal yearly impact to a relatively immune population. My sense is eventually, this will be more of a nuisance to us, much like a troublesome winter “cold” — until then, I hope we can think collectively for a little while longer, especially until we can bring our vaccinations rates, and that of the world’s, to a higher level.